
IQSEC2-related disorder is a rare genetic condition that results from a change in function of a gene called IQSEC2. IQSEC2 is an abbreviation of ‘IQ motif and Sec7 domain 2’, which is a technical description of what the gene codes for. This gene has previously been named BRAG1, MRX1, MRX78, MRX18 and IQ-ArfGEF.
 Genes are the ‘instructions’ that our bodies use for many functions including the control of growth and development. The majority of important genes, such as IQSEC2, code for proteins. Genes can be described as carrying instructions for making proteins that carry out specific tasks. Genes are made from a complex structure called DNA. DNA, and therefore genes, can be described as a sequence of letters but unlike an alphabet, the sequence (or code) only uses 4 letters (G, A, T, C). DNA sequences are incredibly long and include all the information for the thousands of genes included in our ‘genome’ (our complete set of DNA). However, they need to fit inside the microscopic cells that our bodies are made from. DNA is therefore tightly compacted into organized structures called chromosomes.
Genes are the ‘instructions’ that our bodies use for many functions including the control of growth and development. The majority of important genes, such as IQSEC2, code for proteins. Genes can be described as carrying instructions for making proteins that carry out specific tasks. Genes are made from a complex structure called DNA. DNA, and therefore genes, can be described as a sequence of letters but unlike an alphabet, the sequence (or code) only uses 4 letters (G, A, T, C). DNA sequences are incredibly long and include all the information for the thousands of genes included in our ‘genome’ (our complete set of DNA). However, they need to fit inside the microscopic cells that our bodies are made from. DNA is therefore tightly compacted into organized structures called chromosomes.
 Most of our cells normally contain 46 chromosomes, organized as 23 pairs. We usually inherit one chromosome of each pair from our mother and the other from our father. Chromosome pairs are numbered 1 to 22 and the 23rd pair comprises the sex chromosomes, which determine biological sex (whether we are male or female). Females usually have two X chromosomes (XX) and males usually have an X and a Y chromosome (XY). Since chromosomes come in pairs, so do the genes contained within them. We therefore have two copies of each gene in chromosomes 1 to 22, and females (XX), have two copies of each gene on chromosome X. Males have one copy of chromosome X and although chromosome Y does contain some genes that exist on chromosome X, the majority are not present, so males have a large number of genes on the X chromosome that are only present as a single copy. IQSEC2 is located on the X chromosome.
Most of our cells normally contain 46 chromosomes, organized as 23 pairs. We usually inherit one chromosome of each pair from our mother and the other from our father. Chromosome pairs are numbered 1 to 22 and the 23rd pair comprises the sex chromosomes, which determine biological sex (whether we are male or female). Females usually have two X chromosomes (XX) and males usually have an X and a Y chromosome (XY). Since chromosomes come in pairs, so do the genes contained within them. We therefore have two copies of each gene in chromosomes 1 to 22, and females (XX), have two copies of each gene on chromosome X. Males have one copy of chromosome X and although chromosome Y does contain some genes that exist on chromosome X, the majority are not present, so males have a large number of genes on the X chromosome that are only present as a single copy. IQSEC2 is located on the X chromosome.
 The genetic code uses triplets of information to designate which amino acid should be incorporated into the protein. Three base pairs of DNA encode an amino acid. Because the code is ambiguous, some changes in the DNA will not affect the amino acid being encoded. However, some changes will result in a different amino acid being incorporated into the protein. It is humbling to know that only one base pair change (called a point or substitution mutation) can result in a defective protein that causes severe disease. A number of point mutations are known to cause IQSEC2 disease.
The genetic code uses triplets of information to designate which amino acid should be incorporated into the protein. Three base pairs of DNA encode an amino acid. Because the code is ambiguous, some changes in the DNA will not affect the amino acid being encoded. However, some changes will result in a different amino acid being incorporated into the protein. It is humbling to know that only one base pair change (called a point or substitution mutation) can result in a defective protein that causes severe disease. A number of point mutations are known to cause IQSEC2 disease.
There are many other types of mutations which can occur, such as deletions or additions of one or more base pairs to the DNA. Any mutation which changes the protein sequence of the protein has the potential to cause disease; however, not all protein changes are deleterious. To date over 70 mutations have been described that cause IQSEC2 disease however, we do not know which mutations cause more harmful IQSEC2 disease and which mutations are less damaging.
Girls and women (XX): The outcome for girls and women is extremely variable, with the majority being severely or profoundly affected, although a few are known to be mildly affected or not affected at all. In general, girls and women with IQSEC2-related disorder are less severely affected than boys and men. The reason for this is not well understood. For genes located on the X chromosome, the common explanation for less severe symptoms in females is the presence of a second unaffected copy of the gene on their other X chromosome. Likewise, variable symptoms are commonly explained by the natural process of X inactivation, when one X chromosome is randomly ‘switched off’ in each cell during early fetal development (either the one with the variant or the one without). However, IQSEC2 appears to be a complicated gene and it is not yet clear whether or not IQSEC2 is one of the few genes that ‘escapes’ X-inactivation. The common explanation for variable symptoms seen in females may not be valid for IQSEC2. Boys and men (XY): only have one copy of IQSEC2 because they only have one X chromosome in each cell but it is not yet clear whether or not this is the explanation for the fact that they tend to be affected more severely (for example, are more likely to be wheelchair users and have no speech) than girls and women.
The IQSEC2 gene codes for the IQSEC2 protein which is known to interact with other proteins, which are involved in transmission of chemical messages by neurons (nerve cells) in the brain. When the IQSEC2 gene is not working properly, the IQSEC2 protein is abnormal or absent and this interferes with the sending of chemical messages in the brain.
 Neurons produce many long projections (dendrites) which are designed to connect with neighboring cells. Dendrites, which look like tree branches, collect information to bring back to the neuron. One neuron can communicate with thousands of other neurons simultaneously via these projections. IQSEC2 is known to play a role in the normal growth of structures called dendritic spines, which are protrusions that grow out of the dendrites, and are essential for the transmission of electrical signals to the cell body (the central part) of the neuron. Growth of dendritic spines is necessary for the development of a healthy network of interconnecting brain cells and is crucial for learning and memory. The precise function of IQSEC2 is incompletely understood. It is hoped that research will give us a better understanding of this in future.
Neurons produce many long projections (dendrites) which are designed to connect with neighboring cells. Dendrites, which look like tree branches, collect information to bring back to the neuron. One neuron can communicate with thousands of other neurons simultaneously via these projections. IQSEC2 is known to play a role in the normal growth of structures called dendritic spines, which are protrusions that grow out of the dendrites, and are essential for the transmission of electrical signals to the cell body (the central part) of the neuron. Growth of dendritic spines is necessary for the development of a healthy network of interconnecting brain cells and is crucial for learning and memory. The precise function of IQSEC2 is incompletely understood. It is hoped that research will give us a better understanding of this in future.
 The majority of individuals with an alteration in one copy of the IQSEC2 gene reported so far have not inherited it; rather, it has occurred as a new event in them (this is called a de novo gene alteration). De novo gene alterations are random events so they cannot be predicted. IQSEC2 gene alterations have also been reported to have been inherited from mothers who have mild developmental or learning problems or no detectable symptoms.
The majority of individuals with an alteration in one copy of the IQSEC2 gene reported so far have not inherited it; rather, it has occurred as a new event in them (this is called a de novo gene alteration). De novo gene alterations are random events so they cannot be predicted. IQSEC2 gene alterations have also been reported to have been inherited from mothers who have mild developmental or learning problems or no detectable symptoms.
There are at least two reports in the medical literature of siblings with an IQSEC2 gene alteration, which was not present in their parents’ blood samples. This can be explained by a phenomenon called germline mosaicism where the de novo mutation happens after the fertilized egg (zygote) has undergone several divisions. In that case only part of the cells in the body of an individual carries an IQSEC2 gene alteration but the other cells of the body do not (so it would not be detected in a blood sample). It is currently not possible to test eggs or sperm for gene alterations, so there remains a small possibility that the IQSEC2–related disorder can recur in another pregnancy, even when the parents are unaffected and have normal genetic analysis.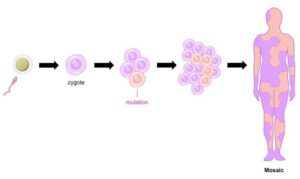
It is for these reasons that parental testing and genetic counselling is recommended for families wanting to have additional children. It is important to emphasize that a child being born with a genetic condition is nobody’s fault. There is nothing either parent did before, during or after pregnancy that could have caused this genetic change. If you have any concerns about having further children, or would like more information, please read our ‘Planning your next child’ guide.
A change in the IQSEC2 gene was first described in a single child in 2013 and since then, several hundred children/people have been described in the medical literature as having a gene alteration in IQSEC2. Genetic testing was once a complicated, costly and time consuming process. Recently, there have been major advances in technology and cost efficiency, that have enabled a more prolific use of genetic testing, so it is likely that increasingly more people will be diagnosed with gene alterations in IQSEC2.
Common features:
- Developmental delay
- Intellectual disability
- Speech and language difficulties or absent speech
- Seizures and epilepsy
- Autism spectrum disorder or autistic-like behaviour
- Hypotonia (low muscle tone/floppiness)
- Developmental regression
Other possible features:
- Ataxic gait (unsteadiness when walking and/or running)
- Drooling
- Unexplained laughter
- Vision problems and/or squint
- Unusual head shape
- Structural brain anomalies on brain scan
- Feeding difficulties
- Gastro-oesophageal reflux
- Constipation
- Sleep disturbance
- Scoliosis (curvature of the spine)
The majority of pregnancies of children with IQSEC2-related disorder reported so far have progressed to term (38-42 weeks) and have been mostly unremarkable. Some children were delivered by emergency caesarean section, but this is also true of children without a genetic disorder.
Some children with IQSEC2-related disorder have feeding difficulties. A few babies have been reported as having gastro-oesophageal reflux or vomiting. For some, the use of medications to help control reflux can be beneficial, for others, nasogastric tube feeding (where a tube is placed through the nose into the stomach) may be required. As children get older, feeding issues can improve, but for some children, difficulties feeding or retaining food causes a gradual but consistent weight loss and a gastric feeding tube (known as a G-tube or PEG (percutaneous endoscopic gastrostomy)) may be recommended (a tube is inserted into the stomach via the body wall through which regular feeds can be administered). Some children also have constipation which may need to be medically managed. Children with IQSEC2-related disorder are expected to have normal growth.
If a child with IQSEC2-related disorder has a developmental disorder such as ASD (autism spectrum disorder) or SPD (sensory processing disorder), this may have an impact on their eating behaviour. Some children may have an aversion to certain foods, whilst others may have a tendency to overeat.
Most children identified so far with IQSEC2-related disorder have been described as having developmental delay. This means that they are delayed in reaching milestones like sitting and walking and have learning disability. All children with IQSEC2-related disorder develop differently and the severity of developmental delay varies. Some children are able to sit and stand shortly after the standard milestone range but most take longer. Most boys will not reach these milestones at all.
The majority of children identified so far have hypotonia, which is low muscle tone causing a child to appear ‘floppy’ and this can have a significant effect on reaching certain milestones. Children may benefit from physiotherapy (also known as physical therapy) and occupational therapy to help them achieve their full potential. Once your child has shown their individual pattern of development it will become easier to predict their longer term possibilities.
The majority of children for whom we have information, have poor gross motor skills but this varies greatly, especially between girls. Most girls learn to walk and run albeit often with some unsteadiness or clumsiness whilst boys may not develop the ability to walk and are described as ‘non-ambulatory’. Hypotonia can affect mobility. Physiotherapists can supply children with equipment like walking frames and wheelchairs and can suggest and perform specific exercises and stretches to aid movement and prevent the development of muscular problems and spinal curvature. Developmental regression (losing skills once learnt) is a feature of this condition. It is not yet known whether lost skills can be re-learnt. The majority of children for whom we have information also require assistance for all areas of daily living.
Intellectual disability (ID) or intellectual development disorder (IDD) are terms used to describe significant limitations in intellectual functioning (measured by
8 IQ scores) and adaptive behaviour (types of behaviour used to adjust to other behaviours or situations). So far, most children reported in the medical literature with IQSEC2-related disorder have also been given a diagnosis of intellectual disability, ranging from mild to profound for girls and severe to profound for boys. Further diagnoses will establish if this is due to the fact that only children who are more severely affected have been offered a genetic test or if all children with IQSEC2-related disorder will develop moderate to profound ID.
Schooling can be a concern for some parents. The vast majority of children with IQSEC2-related disorder will require special needs schooling. Some have very limited intellectual ability. Nonsense and frameshift gene alterations are thought to lead to more significant intellectual disability. In general, intellectual disability is more marked in males.
Speech and language skills can be very variable between children with IQSEC2-related disorder, however marked speech problems are expected. Children are often very delayed in their ability to speak with language being very limited or they do not learn any spoken language but learn other ways to communicate their feelings and needs. It is thought that boys with nonsense or frameshift gene alterations may never learn to talk.
Speech and language therapists can help by assessing communication skills. They can help with speech development and introduce communication devices. They can also help to ensure that whatever your child’s ability, they are supported in achieving their full communication potential.
Although behavioural difficulties have not been fully described for all children reported in the medical literature, behavioural, social and communication difficulties are common in children with IQSEC2-related disorder. Vulnerability in these areas means that children should be monitored and families offered early support.
Autism has been diagnosed in many children with IQSEC2-related disorder. Girls may be more likely to be diagnosed with autism because the more severe intellectual disability in boys may preclude a diagnosis of autism (about half of girls reported to date have been diagnosed with autism). However, severely affected boys may still have some autistic-like behaviour, for example not liking to be touched or a dislike of loud noises. Some children may also have other stereotypic movements (non purposeful movements) such as rocking or hand flapping. Some behaviours may be more prominent when a child is feeling anxious and has difficulties with comprehension and communication.
From birth to at least 3 years of age, most children are routinely screened for developmental milestones. If there are any concerns about a child’s development or behaviour they should be referred for developmental evaluation, which may include an autism assessment.
There is not a ‘medical test’ that can diagnose autism. Children undergo an autism-specific behavioural evaluation usually carried out by a specially trained paediatrician and psychologist. Evaluations will vary according to the age of the child and may be multidisciplinary. A child may be assessed by a speech and language therapist as well as an occupational therapist. Depending on the outcome, further evaluation by a specialist such as a developmental paediatrician, neurologist, psychiatrist or psychologist may be offered or recommended.
Depending on a child’s abilities, joining a social skills group may help with social difficulties, to learn and practise important skills. A parenting course for autism may also help parents to learn behaviour management tools and help to encourage communication and cooperative behaviour in their child to strengthen their emotional wellbeing. Some parents have tried medication to help control their child’s behaviour when it becomes of great concern (such as self-harming or aggression). An occupational therapist may also be able to help with some behaviours by giving your child tools to deal with their sensitivities.
The majority of children with IQSEC2-related disorder have experienced some form of seizure (sudden and unexpected electrical activity in the brain). These can be of different types, from absences seizures (when the child appears vacant and unresponsive for a short period of time) to ‘generalised tonic clonic seizures’ which means that the whole body is involved and, when seizing, alternate stiffening and shaking of the body is seen (dropping to the ground and jerking). More than one type of seizure may be present in the same individual. IQSEC2-associated epilepsy (the tendency to have seizures) is most often diagnosed between the ages of 1 and 3 years. There is marked variation in the persistence of seizures with treatment, some children can have their seizures well controlled with one or two medications, whilst others (mainly boys) have very poorly controlled epilepsy, and can suffer several seizures a day, despite tenacious treatment efforts.
Seizures can cause a lot of worry for families and can be frightening to observe but in the majority of cases they self-resolve, or resolve with medical treatment. If your child has a seizure for the first time it’s important to remove nearby hazards so they can’t hurt themselves and call for an ambulance.
Children who experience seizures may have investigations to check the activity of their brain and to rule out any revisable causes. This may include an ‘EEG’ (electroencephalogram). This is done by attaching stickers to the scalp, which are connected by wires, to the machine used for analysis. Some children have been offered an MRI (magnetic resonance imaging) scan of their brain, to look for structural changes. Different types of structural anomalies have been found including a smaller-than-usual brain.
 Children who suffer from seizures are advised to wear a protective helmet which can prevent them for sustaining serious head injury if they fall during a seizure.
Children who suffer from seizures are advised to wear a protective helmet which can prevent them for sustaining serious head injury if they fall during a seizure.
Children affected by genetic disorders often have higher instances of sleep difficulties than typically developing children. Some families have reported their child with IQSEC2-related disorder finds it difficult to fall asleep at night and early waking and insomnia have also been reported. The reasons for these sleeping difficulties are not yet well understood.
It can be challenging having a child who won’t settle to sleep or who does not have sufficient undisrupted sleep, and it can be very difficult for parents to function well during the day if they have a continuous lack of sleep. There are many interventions that can be put in place to help improve a child’s sleep difficulties. From having a good routine, being aware of strong sensory responses and blocking out natural light in their bedroom to synchronizing their natural ‘body clock’ (circadian rhythm) using ‘light therapy’ (when a child sits near a special light box for a certain amount of time each day to regulate the brains natural sleepiness/wakefulness hormone release) or the use of the hormone melatonin (this is not helpful for all children but may be tried if children have severe sleeping difficulties).
Daytime exercise as well as food and drink consumption may also have an effect on your child’s ability to sleep at night dependent on their age and muscle tone. It has also been suggested that certain food supplements may help with sleeping issues; you may be able to discuss suitability with your doctor.
It is also worth considering that pain, discomfort, allergies and intolerances can all impact on sleep. Medical conditions such as reflux or constipation can also have an effect. In older children, difficulties falling asleep at the end of the day may be associated with anxiety. Sleep onset association disorder occurs when the child associates sleep with a person or something in the environment. This phenomenon may be contributing to sleep difficulties. Unique publishes a freely available sleep guide as part of a practical guide series, it can be found at the following link: https://www.rarechromo.org/practical-guides-for-families.
 A special bed which has a zippered enclosure, such as the Courtney Bed, can help IQSEC2 children and their parents cope with sleeping difficulties. The enclosed bed offers the child a “womb-like” feeling, where they may be more tranquil and likely to fall asleep. The parents can be relaxed knowing the child cannot get out of bed and wander during the night.
A special bed which has a zippered enclosure, such as the Courtney Bed, can help IQSEC2 children and their parents cope with sleeping difficulties. The enclosed bed offers the child a “womb-like” feeling, where they may be more tranquil and likely to fall asleep. The parents can be relaxed knowing the child cannot get out of bed and wander during the night.
There is thought to be an increased chance of scoliosis (curvature of the spine) in children with IQSEC2-related disorder. This is likely due to hypotonia and the muscles not being strong enough to hold the spine straight. Scoliosis can range from very mild and diagnosed incidentally on X-ray to more severe and needing treatment with a back brace or surgery.
Children with IQSEC2-related disorder all look different but some shared facial features have been observed in some children with IQSEC2-related disorder. In some cases, such features are not obvious to a parent or anyone else but may be identified by a paediatrician or clinical geneticist. This is because professionals looking after children with genetic changes are trained to notice physical features that may suggest a child’s difficulties are of a genetic origin. Making a note of these may help establish common features observed in children with the same genetic change and therefore aid diagnosis. Shared facial features that have been identified in some children with IQSEC2-related disorder include deep set eyes, full lips and a frontal upsweep of hair.
Some children with IQSEC2-related disorders have a squint (strabismus, when eyes do not look in the same direction) which can be managed by an ophthalmologist (eye doctor). This is observed in new-born babies but should resolve by 6 months. It is important to identify a squint since it is correctable and can cause damaged vision if not corrected. There may be an increased chance of long sightedness. A few children have been diagnosed with cortical blindness or cortical vision impairment. This means that the eyes themselves can function as expected but the part of the brain that interprets messages from the eyes is not developed properly, so that the child is unable to see.
There have not been any reports of hearing problems in children with IQSEC2-related disorder. It is often difficult to successfully conduct hearing tests in children with severe intellectual disability, however parents do not report any concerns about their child’s hearing.
Most children with IQSEC2-related disorder are expected to enter puberty at the expected time. There is at least one report of a girl who had early-onset puberty but it is not yet known whether or not this was related to her IQSEC2-related disorder since it also occurs naturally in the general population.
We do not currently have much information regarding adults with IQSEC2-related disorder. The eldest people reported in the medical literature are in their 50’s. Unique’s eldest member is 24 years old and the IQSEC2-related disorder support group’s eldest member is in their 40’s.
Other observations
Some children with IQSEC2-related disorder tend to dribble (drool) a lot. There are medications available to help with this (although medication may not work for everybody).
- Children should be under the care of a general or community paediatrician to monitor their health and development.
- Input from the neurology/neurodevelopment teams may also be required.
Seizure activity may need monitoring.
- Health visitors and community nurses play an important role in caring for individuals with IQSEC2-related disorder.
- Monitoring weight gain in infancy is important. Feeding difficulties and reflux may need significant medical support.
- An assessment of special educational needs should be carried out so that extra help can be put in place at school.
- Early input from a speech and language therapist is important.
- Early input from a physiotherapist and occupational therapist is important.
- Sleep disturbance may improve with melatonin.